
At the completion of this article, the reader should be able to improve their management of patients requiring treatment for Ménière’s Disease, including:
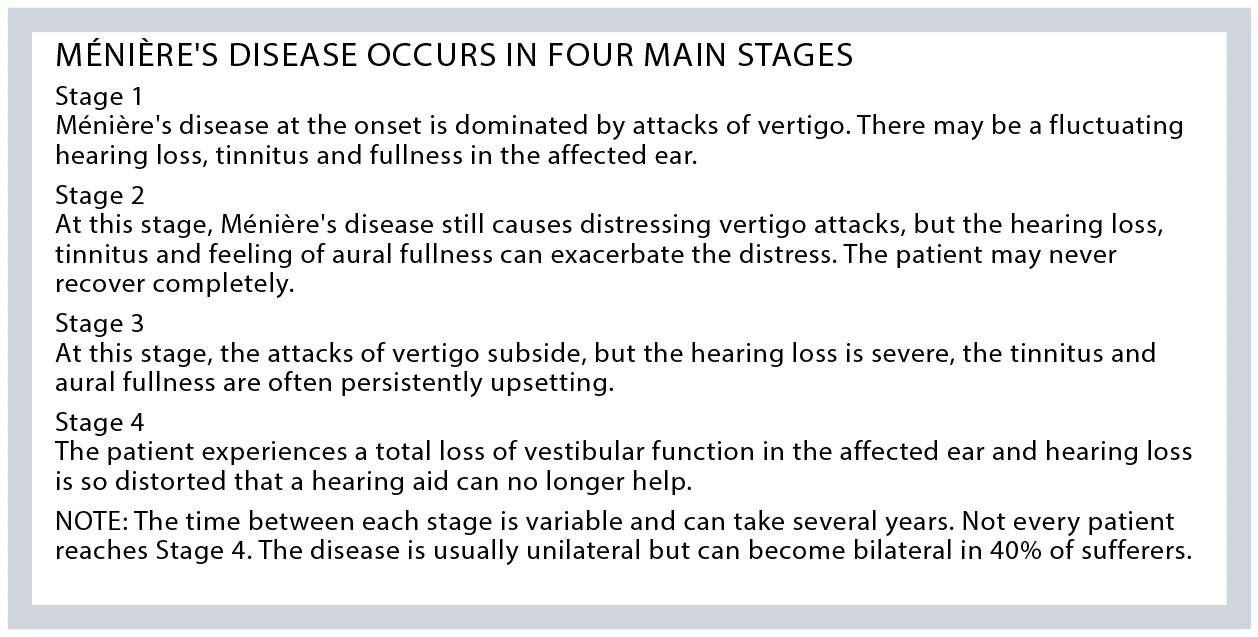
• Know the four stages of Ménière’s Disease
• Be familiar with the ocular symptoms related to Ménière’s Disease
• Be familiar with the anatomy and physiology of the inner ear
• Be able to discuss Ménière’s Disease with their patients, allying fears and explaining available treatment options.

William P R Gibson
AO MD FRCS FRACS
Emeritus Professor of Surgery,
The University of Sydney
Celene McNeill
BSc (Sp & Hg) MA(Aud) PHD audiologist
Healthy Hearing and Balance Care,
Bondi Junction, NSW
While Ménière’s disease primarily affects the inner ear and is typically managed by ENT specialists, vigilant optometrists can play a role in its early detection if they are aware of the condition’s potential ocular manifestations, write Prof WILLIAM GIBSON and Dr CELENE McNEILL.
Ménière’s disease affects about 40,000 Australians. The onset of the condition is usually between 40-50 years of age. The disease can prevent regular work at a time when the sufferer has to support their family. Despite the severity of the disease for the sufferers, curative treatment is still unavailable. Early diagnosis helps to allay fears and provide some simple treatments.
Optometrists are trained to evaluate visual symptoms and ocular health, which can sometimes reveal underlying systemic conditions. In the case of Ménière’s disease, certain visual symptoms or findings during an eye examination may raise suspicion and prompt further evaluation and referral.
Defining Ménière’s disease
Dizziness is the major symptom of Ménière’s disease during its early stages. Characteristically, there is a sensation of rotation, which is called vertigo.
The vertigo is usually associated with nausea and vomiting. The vertigo can be disabling and occur without warning.
Each attack occurs for least 20 minutes and may last for several hours. The vertigo usually occurs in clusters of several attacks with in between periods of remission.
Detection and referral
Diagnosis in the early stage is difficult, but may be suspected if symptoms are present. A hallmark of vertigo is nystagmus. During the sensation of rotation, the eyes deviate quickly in one direction and then more slowly return. For a few days after each attack, the nystagmus may still be detected if ocular fixation is removed. The optometrist may notice that the retina is moving in a jerky fashion if one eye is occluded and a bright light in the other eye prevents ocular fixation.
Questioning your patient about the presence of tinnitus and a sensation of aural fullness can also help to
confirm the diagnosis. The patient should be referred to their family doctor who can prescribe medications. Referral to an audiologist who may be able to demonstrate a fluctuating low frequency hearing loss is very important to reach the correct diagnosis.
Informed referral
A typical referral letter received by the audiologists at the Healthy Hearing & Balance Care clinic from optometrists requests an audiogram. It usually includes reference to the patient’s history of vertigo and the fact that an eye examination prompted suspicion of nystagmus and Ménière’s disease. It’s also important to include the name and contact details of the patient’s GP.
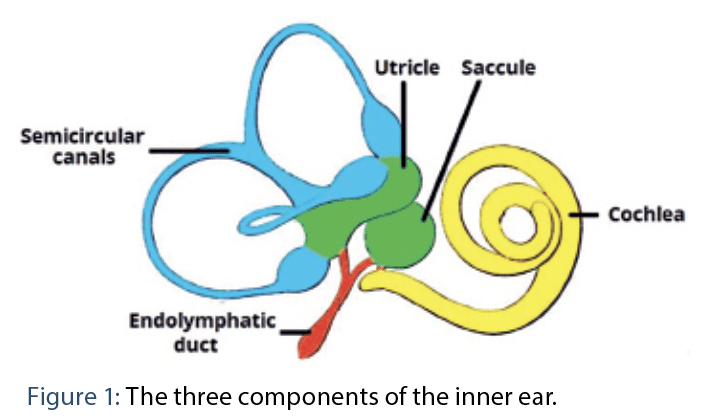
Ear anatomy and physiology
The inner ear (Figure 1) has three main components. The pars superior is the cochlea (yellow) which contains the haircells which respond to the sound vibrations entering via the tympanic membrane and ossicles. The haircells transduce the vibrations into electrical energy to activate the auditory nerve and provide hearing.
The pars inferior consists of three semi-circular canals (blue) which measure head movements in all directions and keep the eyes on target. Loss of bilateral semicircular canal function results in opisthotonos, an illusion that the surroundings are bobbing up and down. The lateral semicircular canal is dominant in humans and alterations in its output results in horizontal nystagmus.
The semicircular canals arise from the utricle (green) which contains the otolith organ which provides the sensation of sideways and back and forth movements. Pieces of this organ called otoliths can displace into the semicircular canals, most often the posterior semicircular, which can cause benign paroxysmal positional vertigo (BPPV). BPPV gives a sensation of spinning which lasts a few seconds on certain head movements. There is also another organ within the otolith ‘the saccule’ (green) in the pars inferior which provides the feeling of vertical movements.
The pars superior and the pars inferior are joined by the ductus reuniens which connects to the saccule. The saccular duct leads to the endolymphatic sinus which also connects via the utricular duct to the utricle. There are two types of fluid within the inner ear: the endolymph and the perilymph. The membranous labyrinth contains endolymph which bathes the haircells in the cochlea and fills the pars inferior. Excess endolymph is called endolymphatic hydrops and is a feature of Ménière’s disease. There is a mechanism called longitudinal drainage which can take the excess endolymph to the endolymphatic sac (red) for removal. For example, when there is an infection within the inner ear, excess endolymph is produced and then drained to the endolymphatic sac removing noxious agents away from the haircells which cannot regenerate.
The pathophysiology of Ménière’s disease
The original description of the disease was by Prosper Ménière in 18611 who recognised that the symptoms were due to an inner ear disorder. It was in 1938 that Hallpike and Cairns,2 and independently Kamakawa,3 described endolymphatic hydrops histologically. It is likely that endolymphatic hydrops relates to the loss of hearing, tinnitus and sensation of aural fullness. An increase in endolymphatic hydrops is probably the cause of the attacks of vertigo.
In ears affected by Ménière’s disease, the passage of endolymph down endolymphatic duct is restricted. This can be due to narrowing of the surrounding bony vestibular aqueduct, but other causes are possible.
There are two main theories of the cause of the attacks of vertigo. Schuknecht4 proposed that ruptures of the delicate Reissner’s membrane within the cochlea caused a mixing of perilymph and endolymph reducing the afferent neural impulses from the semicircular canals until the rupture was repaired.
An alternative theory5 is that when the endolymph drains from the cochlea it cannot pass freely towards the endolymphatic sac and some cochlea endolymph passes into the utricle stretching the haircells within the cristae of the semicircular canals.
Diagnosis
The diagnosis depends on the clinical history of the patient and supportive tests.
The American Academy of Otolaryngology and Head and Neck Surgery (AAOO-HNS) provided the following two categories of the diagnosis of Menière’s disease in 2020.
• Definite MD: Two or more spontaneous attacks of vertigo, each lasting 20 minutes to 12 hours. Audiometrically documented fluctuating low to midfrequency sensorineural hearing loss (SNHL) in the affected ear on at least one occasion before, during, or after one of the episodes of vertigo. Fluctuating aural symptoms (hearing loss, tinnitus, or fullness) in the affected ear. Other causes excluded by other tests.
• Probable MD: At least two episodes of vertigo or dizziness lasting 20 minutes to 24 hours Fluctuating aural symptoms (hearing loss, tinnitus, or fullness) in the affected ear. Other causes excluded by other tests.
MRI is now the test which excludes other causes.
Supportive tests
Pure tone audiometry can indicate the stage of the disease. Initially, in Stage 1, the audiogram can fluctuate back to normal levels. A low and mid frequency sensory loss is typical in Stage 2 and in Stage 3, the hearing loss is severe, affecting all frequencies.
• Vestibular tests can show a loss of function in the affected ear. Vestibular function loss may not be evident until Stage 2 and 3. Classically, the caloric test when warm and cool water is poured into the ears and the affected side gives a lesser response. More recently other tests can be undertaken. The video head thrust (vHIT) tests show the function of each of the semicircular canals. The ocular and cervical myogenic tests can show abnormalities of the utricular and saccular otolith organs.
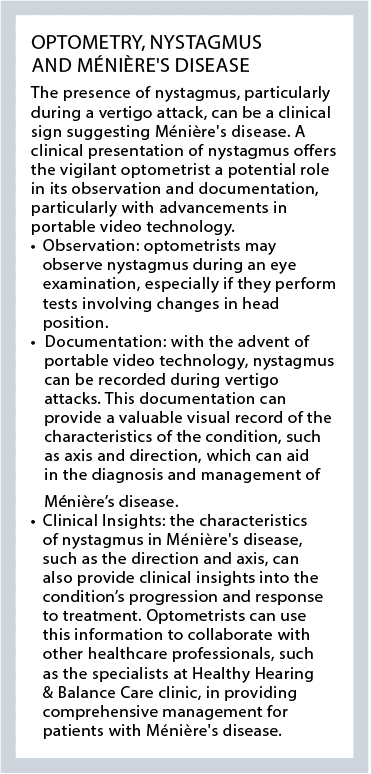
• Nystagmus during Ménière’s attacks is usually horizontal with the fast phase beating to the contra-lateral ear during the attacks and to the affected side during the recovery period. More recently, the advance of portable video technology use in mobile phones has allowed eyecare providers, and patients, to record evidence of nystagmus showing different axis and directions during vertigo attacks.
The following tests are available at major public hospitals and also in specialist audiology centres such as Healthy Hearing & Balance Care clinic.
• Electrocochleography is the recording of the electrical responses in the cochlea to sound. The potentials can be distorted in the presence of endolymphatic hydrops. Electrocochleography is most accurately obtained by a needle electrode placed through the tympanic membrane (transtympanic). As this is an invasive test, it is likely to be replaced by the Magnetic Resonance Imaging (MRI).
• MRI is likely to become the test for showing the presence of endolymphatic hydrops. The contrast agent Gadolinium (Gd) remains in perilymph and only slowly enters the endolymph compartment. There are serious complications to administrating too high a dose of Gd intravenously, so often it was administered by a transtympanic injection so that the Gd infuses into the perilymph from the middle ear.
Because of the advances in MRI imaging and with the use of head coils, the Gd can now be given at reasonably safe levels intravenously. The MRI in a normal cochlea shows the endolymph compartment as a black area where there is little Gd but when there is endolymphatic hydrops, the size of this black area is increased.
Patient education
While Ménière’s disease can be challenging to manage, optometrists can explain to their patients that there are effective treatment options available to help improve sufferer’s quality-of-life.
Above all, correct diagnosis and reassurance that Ménière’s disease is not a brain disorder and not life threatening is vital.
During acute vertigo episodes, Zofran (ondansetron) 4-8mg helps control vomiting and a vestibular sedative can be combined. Severe episodes may need paramedical assistance and a vestibular sedative can be administered intramuscularly as oral medication would be vomited.
If there are clusters of frequent attacks, steroids given orally or injected into the ear may be needed.
For ongoing support between attacks, reduction of salt and increased water intake, and sometimes diuretics to reduce fluid in the inner ear, help. Long term use of prochlorperazine (Stemetil) or similar medications are discouraged because of side effects.
If the attacks of vertigo are frequent and severe, treatment to reduce the strength of the vestibular function are available. A series of gentamicin injections injected into the middle ear can be effective. Surgical treatments include endolymphatic sac surgery. Vestibular nerve section destroys all the balance function in the ear which certainly stops the attacks but has some long-term balance side effects.
Treatment of hearing loss and tinnitus
There is no medication to improve hearing loss or tinnitus. However, help is available using properly-fitted hearing aids. The hearing aid needs to be adjustable as the hearing can frequently vary, especially in Stage 2. Tinnitus is due to circuits in the mid brain becoming altered. Tinnitus in Ménière’s disease is usually appeased by an alternative sound reaching the brain. Hearing aids can be very successful to reduce tinnitus perception and improve overall hearing.
If the sufferer reaches Stage 4, hearing aids can no longer help. Fortunately, a cochlear implant is often very effective for both hearing improvement and tinnitus reduction.
A hypothetical case history and referral
John is 45 years old with a young family. One day, he suddenly becomes very dizzy and is vomiting. His wife calls an ambulance fearing the worst. He is taken to hospital, given medication and then allowed home with a suggestion he goes to his family doctor.
Unfortunately, the attacks continue every few weeks and his vision seems disturbed. He goes to his optometrist who reassures him that his eyesight has not changed but has noticed that he has some nystagmus as his retina moves jerkily when his optic fixation is removed.
The optometrist has some knowledge of Ménière’s disease and asks if he has any hearing loss, tinnitus or sensation of ear fullness. The optometrist suggests he has some testing by an audiologist. The results are then given to the general practitioner who has arranged an MRI to exclude the presence of a brain tumour.
The diagnosis has been established, but the clusters of attacks continue. John has had to relinquish his job as he cannot reliably attend work. The general practitioner may refer John to an ENT specialist who deals with Ménière’s disease. Audiological and vestibular testing is required to determine best management options.
After appropriate treatment, the vertigo becomes manageable but there is still the worry of declining hearing, and the tinnitus can be very frustrating. The audiologist can provide ongoing support even if a cochlear implant is eventually required.
Summary
The diagnosis of Ménière’s disease in the early stages is not easy. Often the first attacks lead to trips to hospital where medication is given to ease the vertigo. The sufferer may be terrified that a brain tumour has caused the vertigo. Early diagnosis of Ménière’s disease provides reassurance and can lead to useful treatments.
Optometrists can also provide support and guidance to patients by referring them to audiologists and ENT specialists for further evaluation and treatment. And finally, by educating patients about their condition and the available treatment options, optometrists can empower them to take an active role in managing their health and improving their quality-of-life despite the challenges posed by Ménière’s disease.
More reading
Insights from an Australian gonioscopy workshop – Part 2
Gonioscopy primer: Insights from a gonioscopy workshop (Part 1
Real-world insights into managing severe keratitis in dry eye disease with Ikervis
References
1. Ménière P. M Mémoire sur des lésions de l’orielle interne donnant lieu à des symptômes de congestion cérébrale appoplectiforme. Gaz Méd Paris 1861; 16 :597-601.
2. HallpikeC, Cairns H. Observations on the pathology of Menière’s Disease. JLaryngol Otol 1938; 53:624-54.
3. Yamakawa Y. Über die pathologische Veränderung bei einem Meniere- Kranken J. Otorhinolaryngol Soc Jpn 1938; 884:2310-12.
4. Schuknecht H: Correlation of pathology with symptoms of Menière’s disease. Otolaryngol Clin North Am 1968; 1: 433–38
5. Gibson WP: Hypothetical mechanism for vertigo in Menière’s disease. Otolaryngol Clin North Am 2010; 43: 1019– 27.



{kind=link}